
Minnesota’s hospitals are operating in a moment of unprecedented strain — not just financially, but structurally.
About than two-thirds of patients treated in Minnesota hospitals are covered by programs that do not fully pay the cost of care. At the same time, recent federal policy changes — including reductions in Affordable Care Act subsidies and tighter Medicaid eligibility under the One Big Beautiful Bill Act — are expected to leave tens of thousands of Minnesotans uninsured or underinsured.
When coverage disappears, care does not. Emergency rooms remain open. Specialists continue to treat. But the financial burden shifts — to hospitals, to communities, and ultimately to employers and families. Care never runs out. Only the money does.
Meanwhile, the workforce shortage is intensifying. According to the Minnesota Department of Employment and Economic Development, nearly 1 in 10 pediatrician positions and nearly 1 in 8 family practice positions were vacant in 2025. In some behavioral health categories, vacancy rates approach 40%.
The question facing Minnesota is not whether hospitals matter. It is whether we will sustain the statewide system of care that Minnesotans depend on.


Minnesota has a wide array of hospitals, ranging from small, municipal hospitals to global health systems. Nearly all are non-profit, governed by boards of volunteer trustees that represent their communities, from small towns to multinational patient populations.
The hospitals fall into a broad system of categories, generally defined by federal and state regulation – and some hospitals may fit in more than one category.

Critical Access Hospitals
These are small hospitals, limited by Centers for Medicaid and Medicare Services (CMS)* to 25 beds and a four-day average stay. They are often considered “rural” hospitals. Their defining feature is their location: at least 35 miles from another hospital and the only hospital in practical driving distance for patients in the most need. Minnesota has 76 such hospitals, the 4th most in the U.S., and they span from the Rainy Lake Medical Center in International Falls to the United Hospital District in Blue Earth.

Prospective Payment System Hospitals
These are larger hospitals, paid by CMS* under the inpatient prospective payment system (PPS), which is built on a flat-rate reimbursement based on average U.S. charges for specific diagnoses. 49 Minnesota facilities are PPS hospitals. St. Luke’s in Duluth, Mayo Clinic in Rochester, St. Cloud Hospital, and Mercy Hospital in Coon Rapids are all examples.

These provide only emergency care and do not offer inpatient services. Minnesota has only one, in Mahnomen. It is also the only such hospital in the Upper Midwest. This is a new designation as of 2020, and is meant as an alternative to closing a hospital.

Health Systems
More than half of Minnesota’s hospitals are affiliated with nine larger networks comprised of multiple inpatient care providers, including Allina Health, Aspirus Health, Avera Health, Catholic Health Initiatives, CentraCare Health System, Children’s Minnesota, Essentia Health, HealthPartners (including Park Nicollet Health Services), Lake Region Healthcare, M Health Fairview, Mayo Clinic, North Memorial Health, Ridgeview, and Sanford Health.

Academic Health Centers
These are large hospitals integrated with medical schools. Minnesota’s biggest academic health center is in Minneapolis, part of the M Health Fairview system. The University of Minnesota also has medical school campuses co-located with the Mayo Clinic in Rochester, CentraCare in St. Cloud, as well as a stand-alone Duluth campus.

“Safety Net” Hospitals
This isn’t a formal designation, and all hospitals are safety nets for their communities. Often, this term is used to designate hospitals that provide about half of all inpatient stays for uninsured patients or Medicaid beneficiaries. HCMC considers itself a safety net hospital.

Pediatric Hospitals
These are hospitals that specialize in care for children, like Children’s Minnesota, Gillette Children’s and the M Health Fairview Children’s Hospital.

Specialty Hospitals
These are hospitals that typically focus on a limited range of patients and are not generally open to the public. They include hospitals like the Minneapolis VA Medical Center, Indian Health Services hospitals, the Capitol Park Mental Health Hospital in St. Paul, and the Anoka Metro Regional Treatment Center. Minnesota also has only two private hospitals, Regency Hospital, in Golden Valley and Prairie Care in Brooklyn Park. (The Minnesota Security Hospital in St. Peter is not licensed as a hospital.)
*The Centers for Medicaid and Medicaid Services (CMS) is a federal agency that oversees and regulates the Medicare and Medicaid programs. CMS rules, definitions, and finances are generally the defacto standard in U.S. health care.
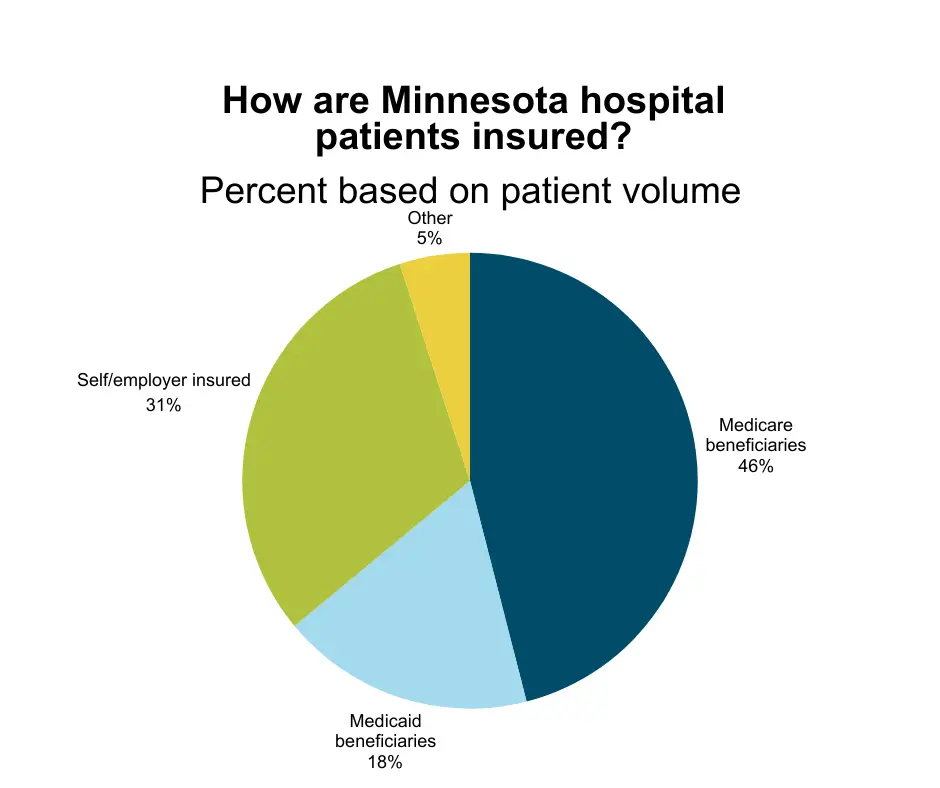
You may be surprised to learn that care for most patients in Minnesota hospitals is paid for by taxpayers.
Two historic programs, Medicare and Medicaid pay for care for nearly 2/3 of Minnesota hospital patients. Medicare is funded by federal taxpayers. Medicaid is paid for by both federal and state taxpayers.
What you also may not know about Medicare and Medicaid: They don’t cover the actual cost of care. Medicare reimburses hospitals at a rate of 82 cents on the dollar, and Medicaid at 79 cents on the dollar.
Hospitals also provide hundreds of millions of dollars of uncharged “charity care” annually, and write off hundreds of millions more in unpaid bills as uncollectable debt — debt which, by hospital agreements, isn’t reported to credit agencies.
Also, thousands of patients get care at hospitals that is not billed to any patient or payer. They may be stabilized in an emergency department and waiting for an inpatient bed, headed to a nursing facility or waiting for admission to mental health treatment – getting hospital care that is needed, like food and monitoring – but care that can’t be billed as medical services.
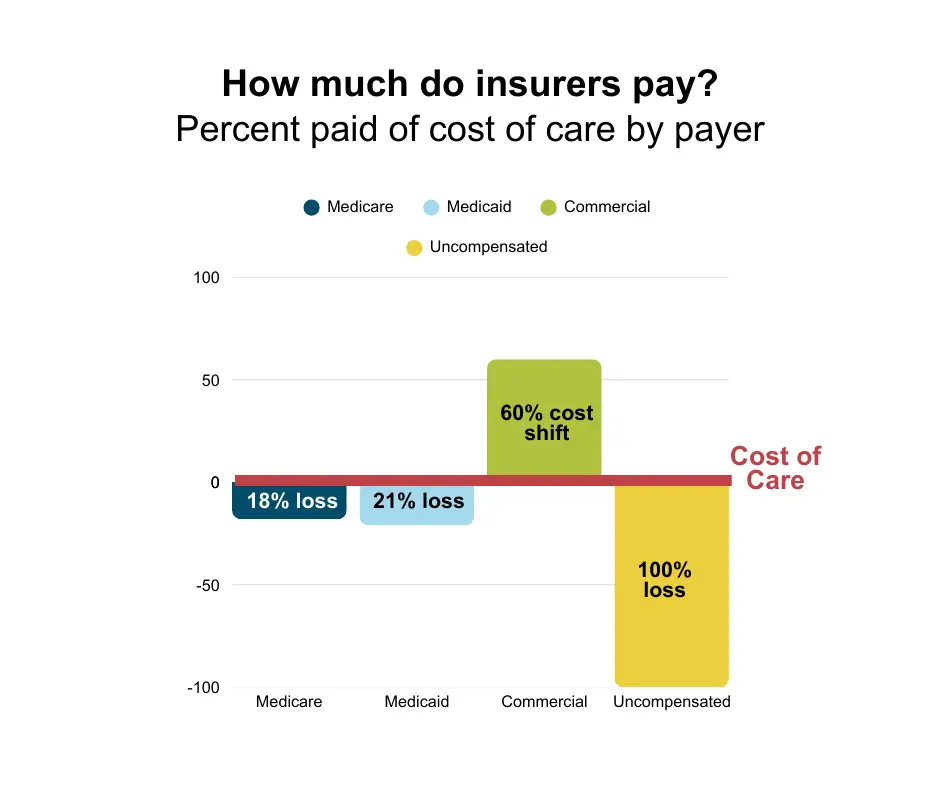
Hospitals try to close the financial gap between costs and reimbursements in a variety of ways. Principally, it is by shifting costs to other major payers — private health insurance, often sponsored by employers.
Hospitals also rely on a whole host of other revenue streams, including proceeds of sales from drugs in the federal 340B drug discount program, workforce development and training programs, public health spending, investment income and charitable donations, just to name a few. These are important, but key supports that make payroll and keep the lights on and the doors open at Minnesota hospitals.


Minnesotans enjoy what consistently ranks as some of the best health care in the world, the vast majority from hospitals and the clinics, ambulatory care centers, labs, and treatment facilities affiliated with health systems.
Minnesota also has the seventh-highest life expectancy in the U.S., compared to the 11th highest median household income in 2024, a testament to the value health care providers bring to Minnesotans.
Minnesota providers are leaders in telehealth, public health, addressing the social determinants of health, and community involvement. Mobile vaccination campaigns, food assistance, fitness facilities, community clinics, mobile mammography, and housing supports are just a few examples of the ways Minnesota hospitals invest into keeping patients healthy. – preventing the need for ambulances, emergency rooms, and patient beds. The best care, we all know, is the care that you don’t have to have.
Scalpels, scanners, and stethoscopes don’t provide care: people do.
More than 151,000 employees ensure excellent care is available at Minnesota hospitals and health systems 24 hours a day, 365 days a year.
Care teams are hospitals’ biggest investment. Hospitals pay more than $13.4 billion in payroll and benefits – in fact, many are benefit-eligible after working just 24 hours a week. Hospital and health system nurses in Minnesota are consistently #1 or #2 for cost-of-living adjusted wages in the U.S., and employee development, diversity and retention remain a top priority for hospitals.



Minnesota is also desperately in need of support workers that help move patients out of acute hospital care, like personal care attendants and certified nursing assistants in skilled nursing facilities. In 2024, there were 9,949 vacant positions for health care support occupations. Overall, health care has the highest vacancy rate of any industry.
Demographic changes mean that by 2035, meeting health care workforce needs could demand three quarters of new workers go into health care – a highly unlikely scenario. That underlines the essential need to gear up workforce development now.

Minnesota took a key step forward in 2025, as CentraCare opened a new University of Minnesota Medical school campus, with an initial class of 24 future doctors.

A Looming Insurance Crisis
Changes to federal law will impose new work reporting requirements on thousands of Medicaid recipients in in Minnesota in 2027. As a result, many individuals may lose coverage due to administrative barriers. As these uninsured individuals resort to the emergency room for any necessary medical care, hospital uncompensated care is estimated to increase by 21.5%.

A Mental Health Crisis
There are not nearly enough mental health and addiction treatment providers. More than 800,000 people in Minnesota have a mental health condition, and almost every county has an area with a mental health shortage. Hospital emergency departments are not a suitable or safe substitute for specialized care.

Federal 340B Drug Pricing Program
Proceeds from sales of discounted drugs earn hospitals more than $1 billion annually. Elimination of discounts, restrictions on participation, and a sunset on a state mandate to include a wider range of pharmacies will substantially reduce this vital and flexible funding source.

State Directed Payments
Congress has barred Minnesota from enacting a Medicaid matching program in effect in more than 40 other states. The new ban on directed payment programs may cost Minnesota hospitals approximately $1 billion annually in reimbursement for care for low-income Minnesotans.
The Community Hub offers event registrations and other members-only content.
The MHA Portal provides a single point of entry to our data submission applications.
Changes are coming to the MHA Portal. New information will be available here soon.
Need help logging in? Contact us.